Fallserie





10-jähriges Mädchen — Larsen-Syndrom
3 Folien
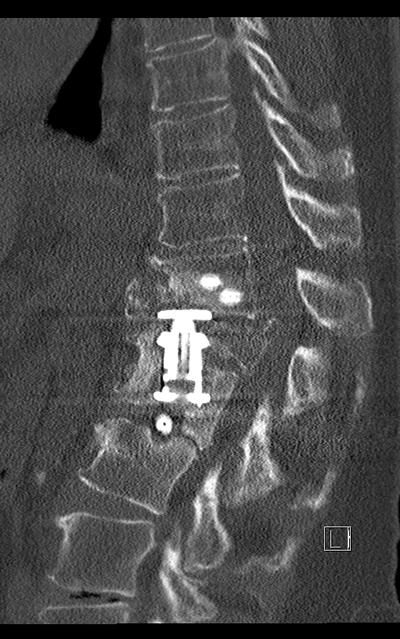
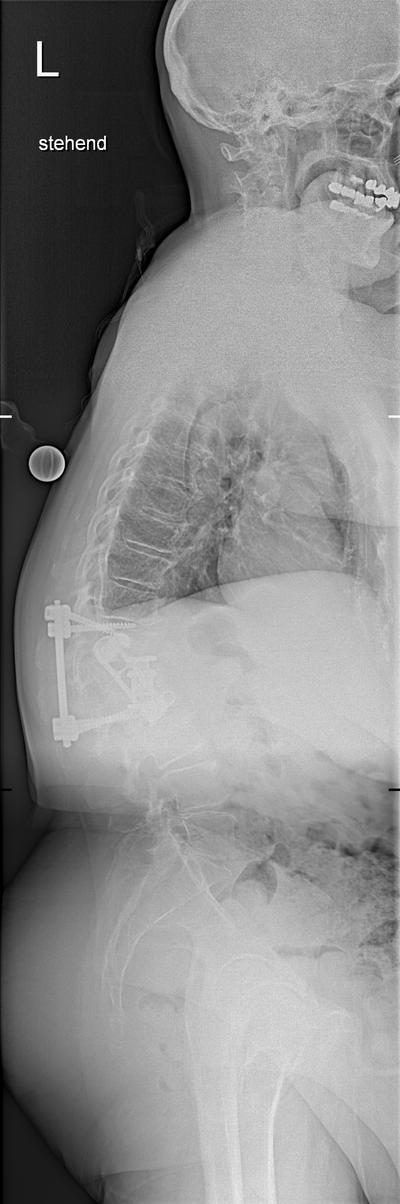
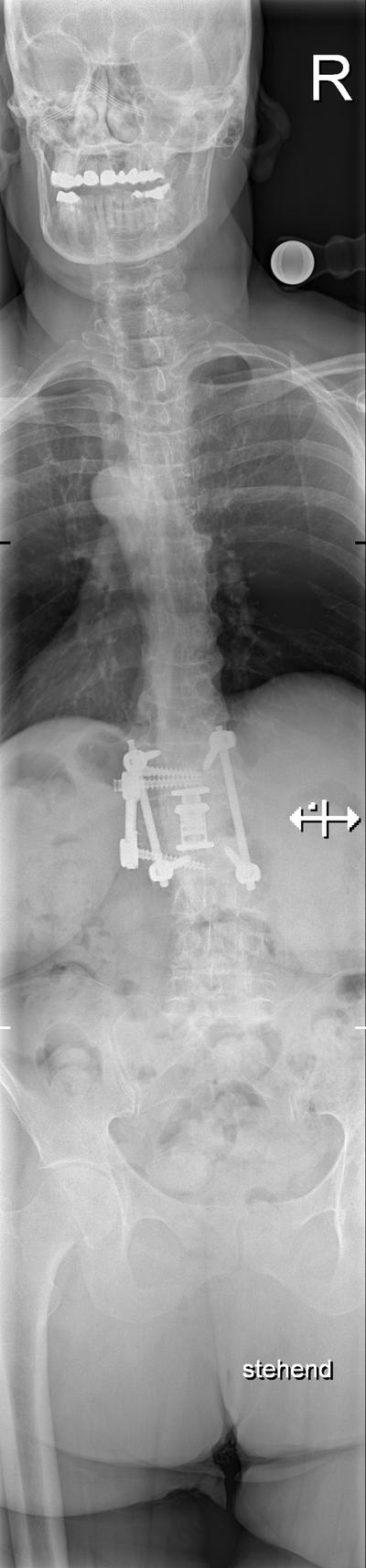
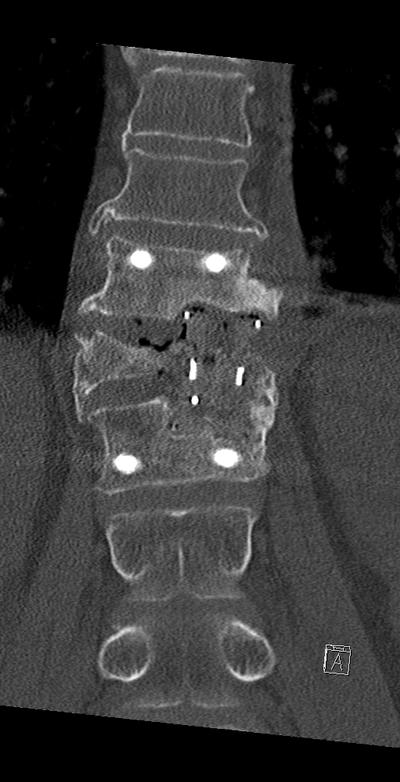
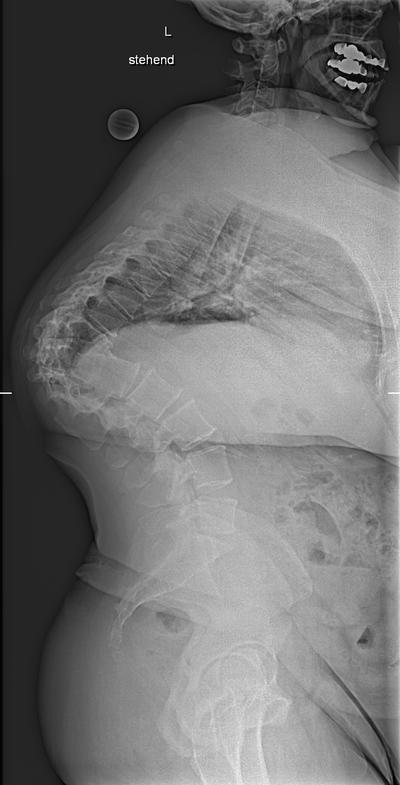
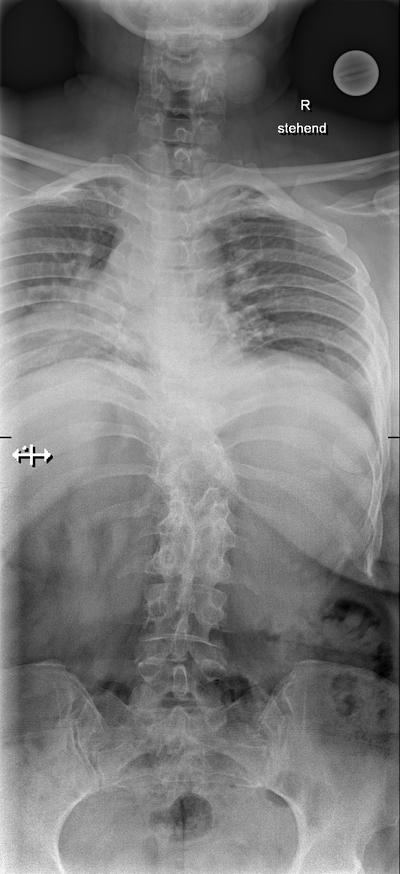
10 y.o. girl, Larsen syndrome (feature no bony connection between the posterior elements and the vertebral body), progressive tetraparesis, loss of ambulation
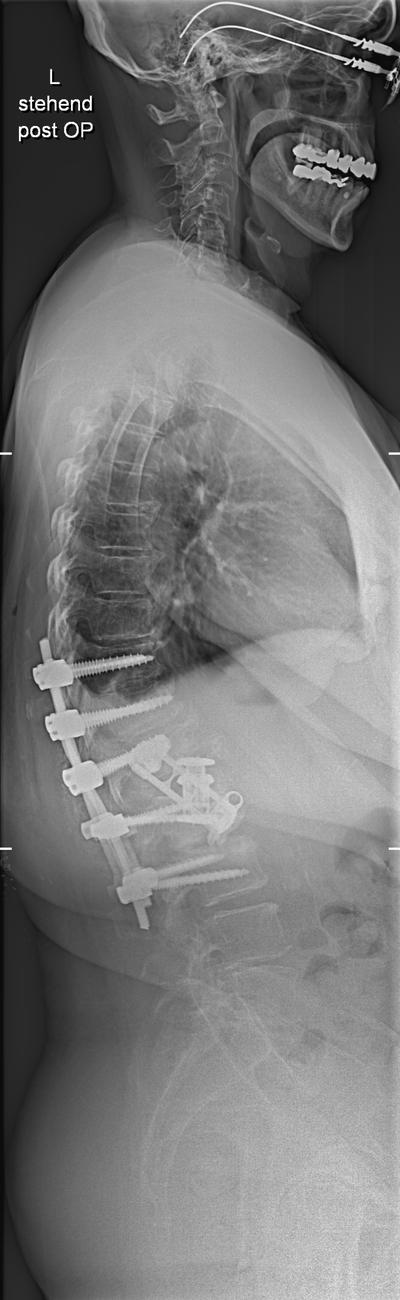
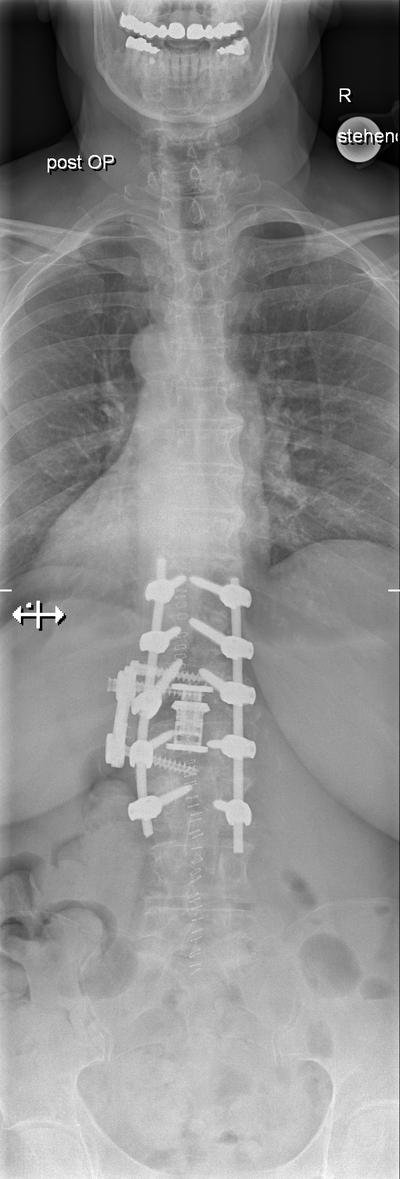
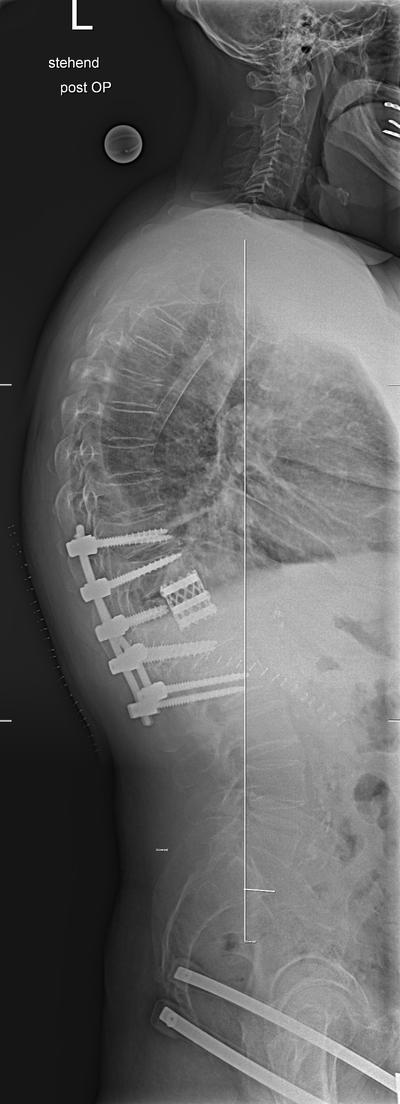
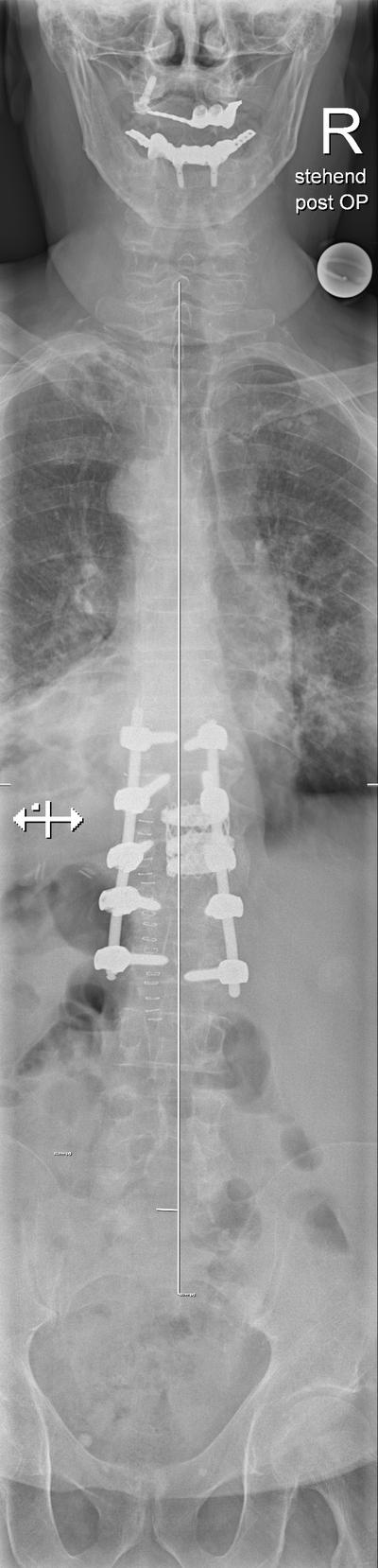
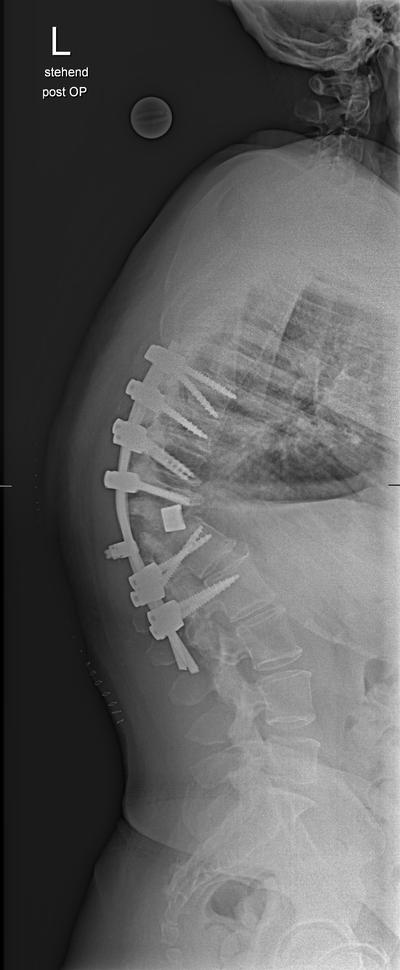
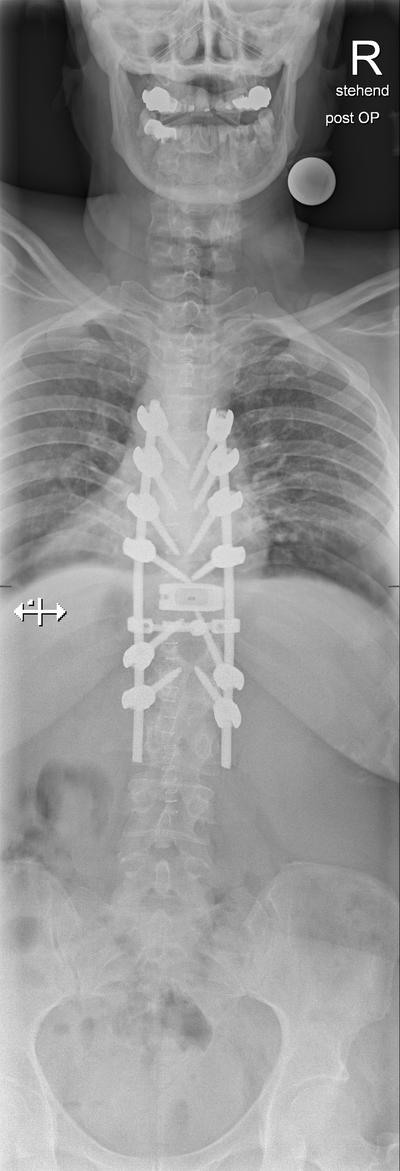
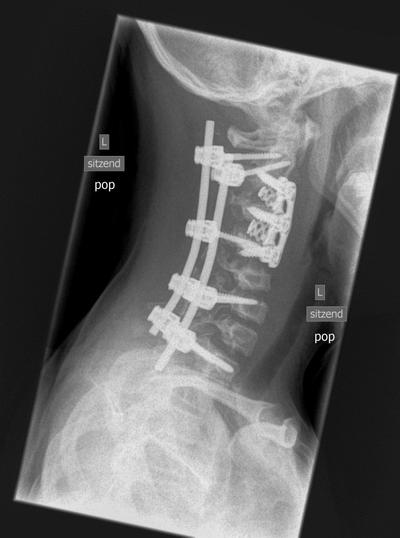
After preoperative halo-traction and dorsal decompresion and instrumented fusion C2- T1
After ACDF C2-4. Symptom release with ambulation again possible