Fallserie


























































Kombinierter Zugang bei idiopathischer Skoliose (AIS)
21 Folien
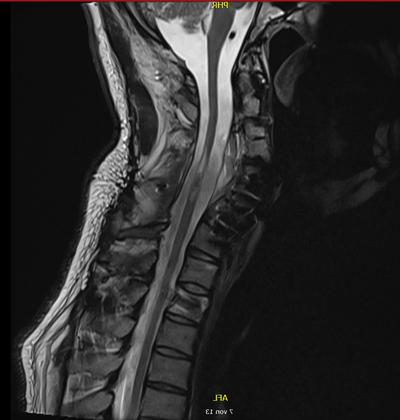
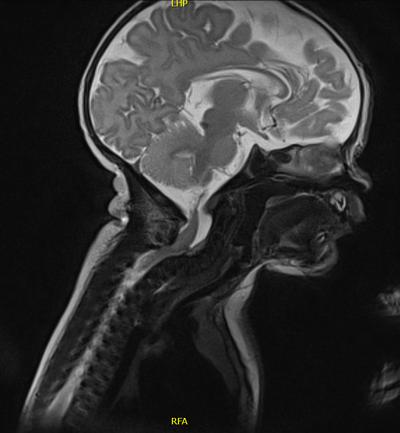
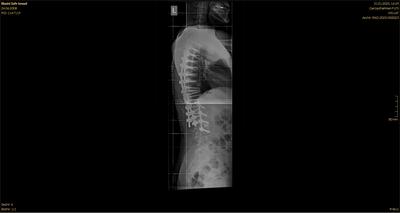
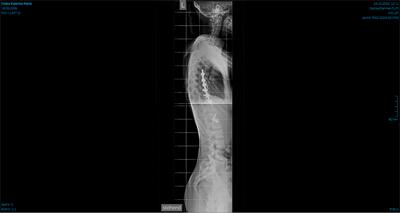
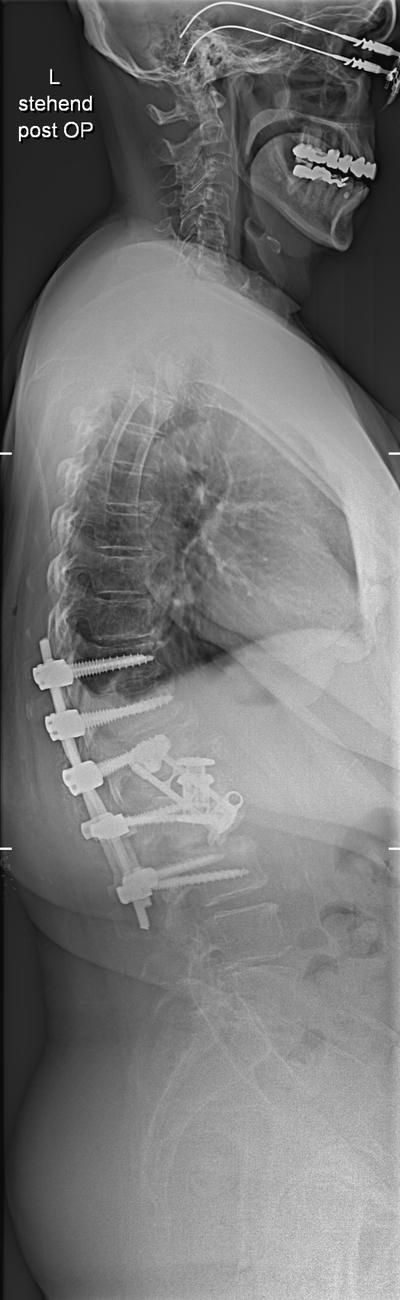
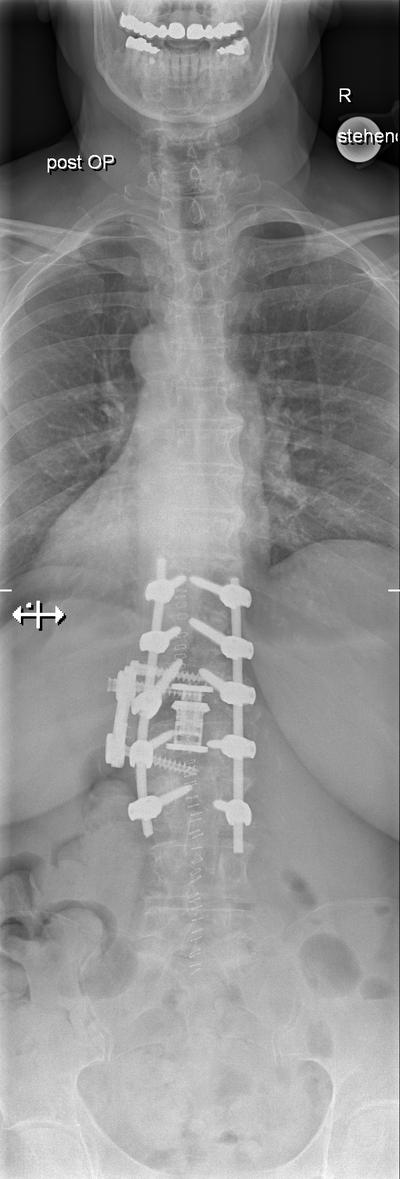
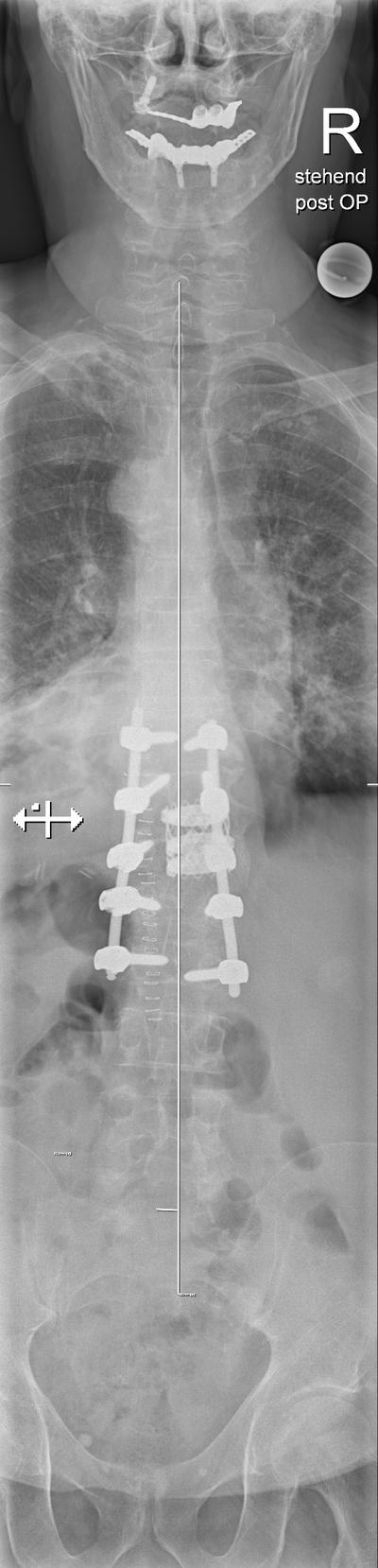
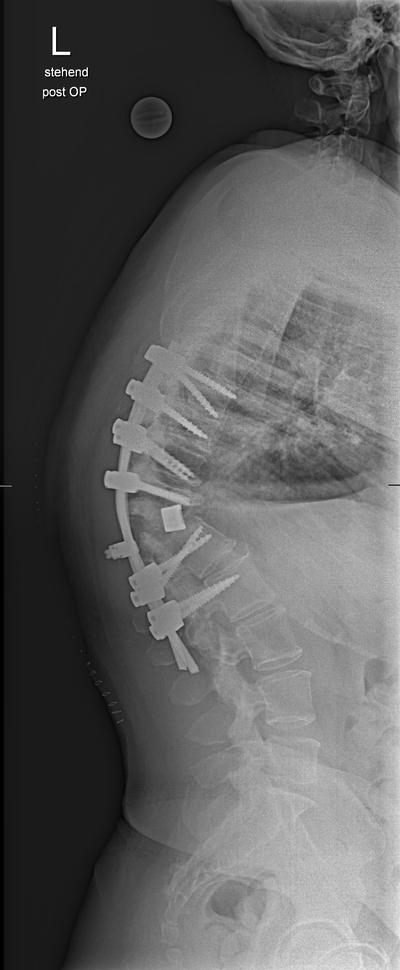
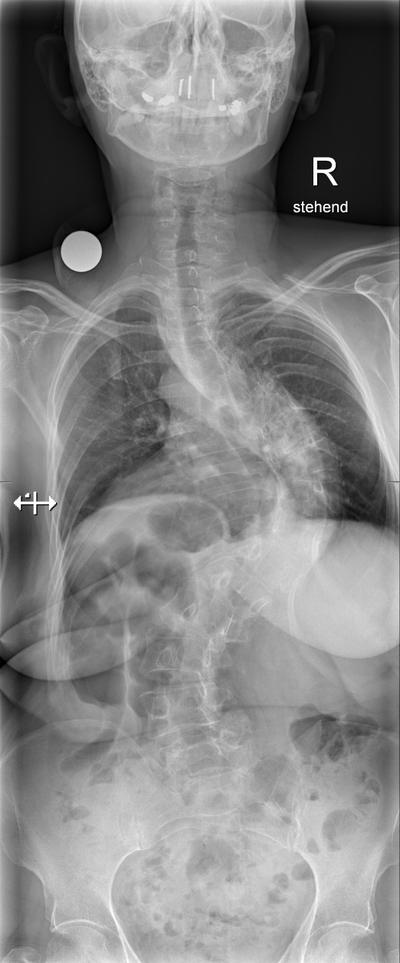
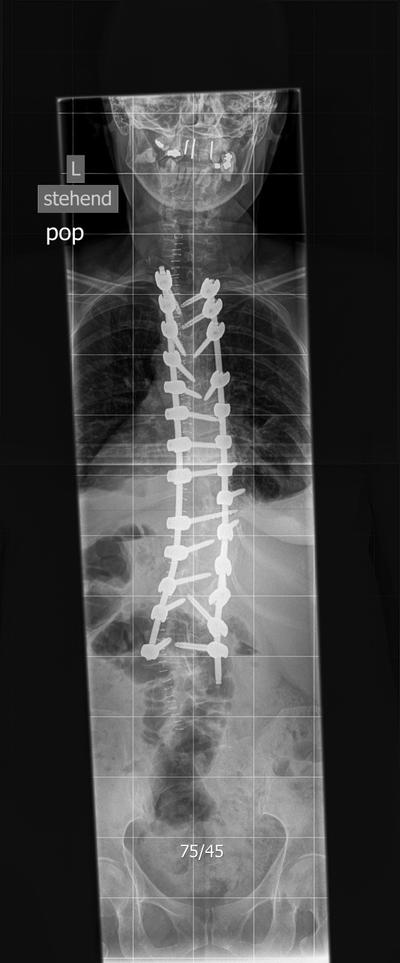
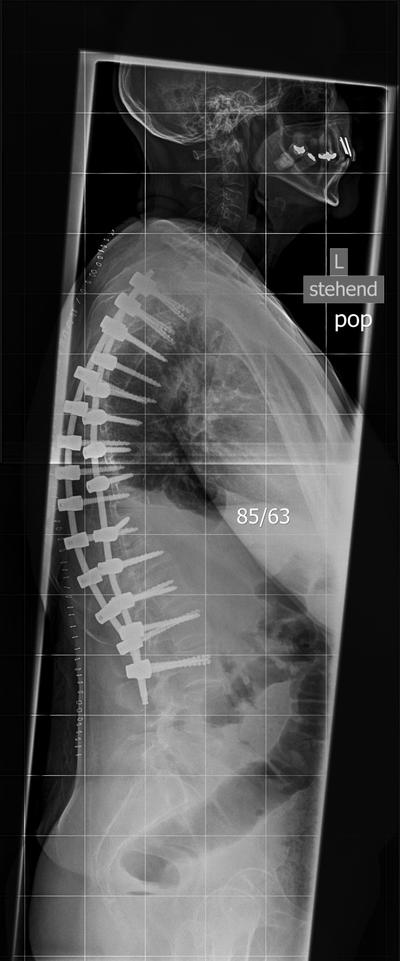
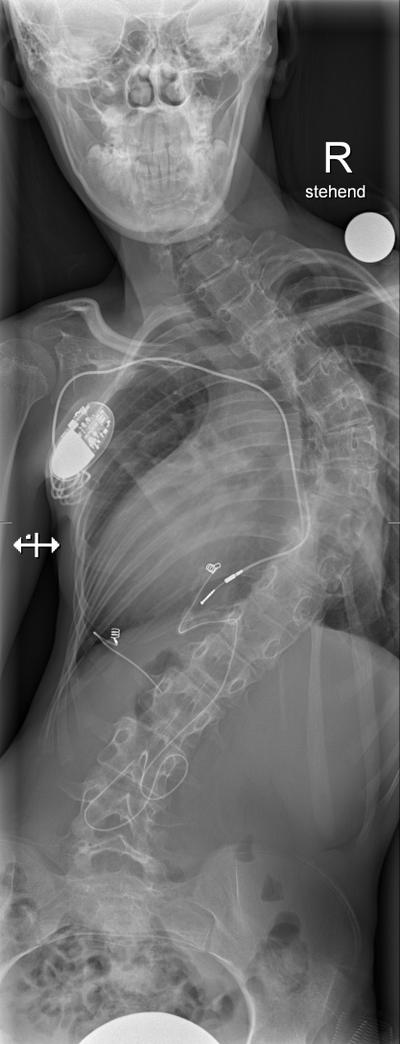
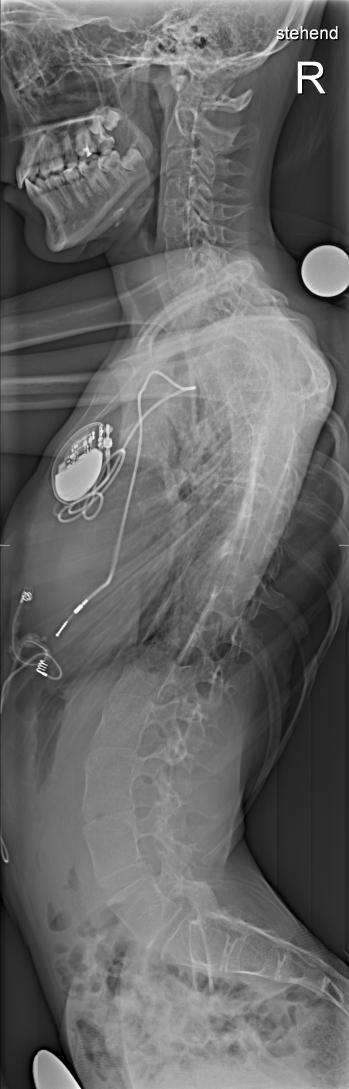
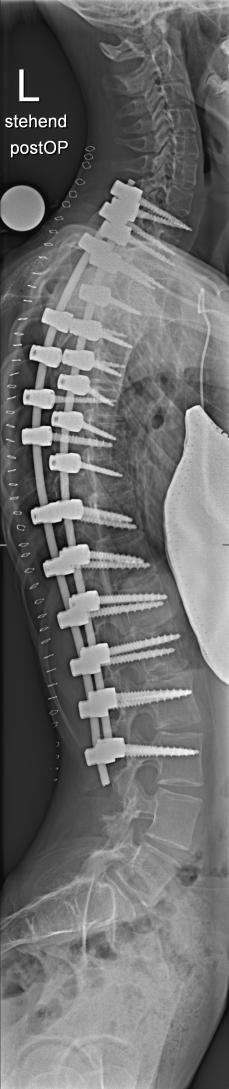
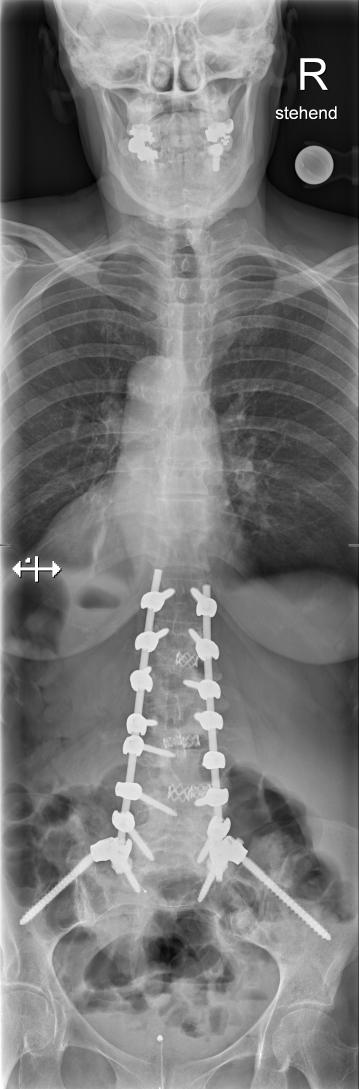
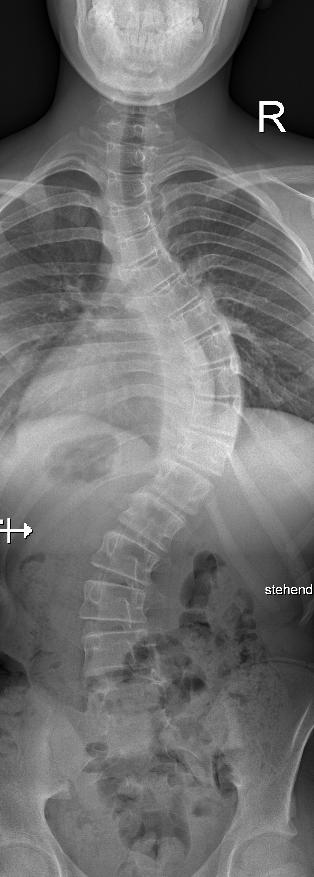
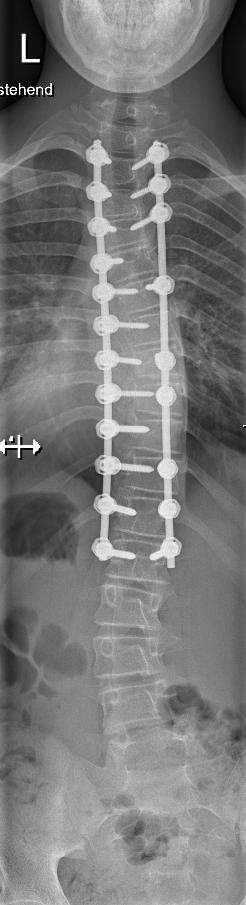
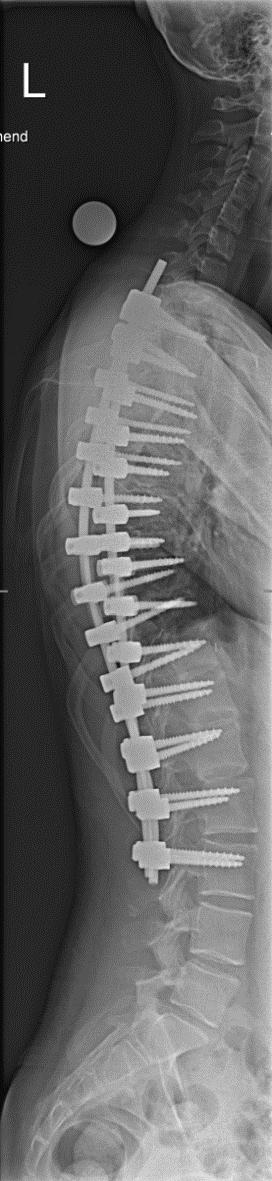
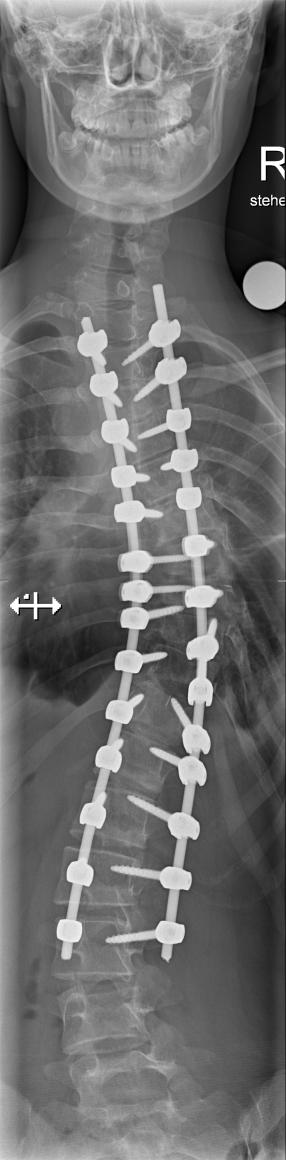
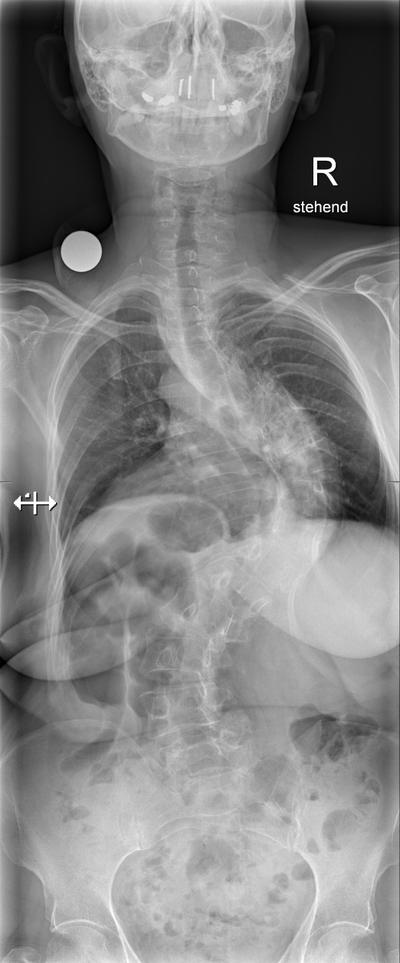
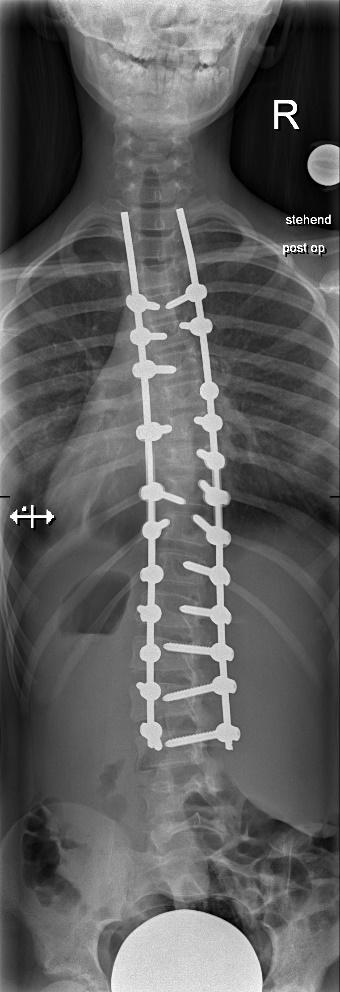
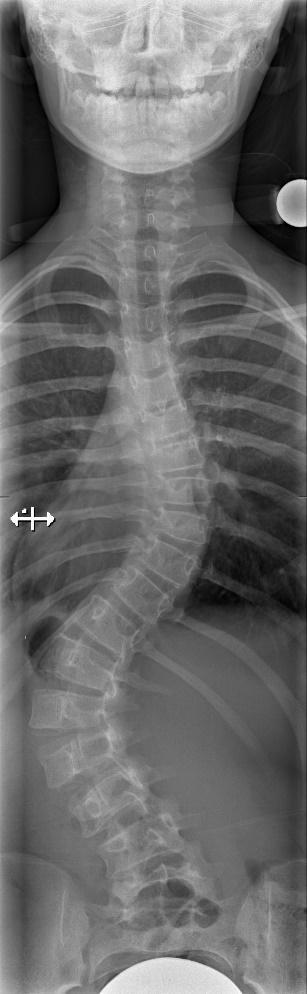
Flat Back following Posterior Correction
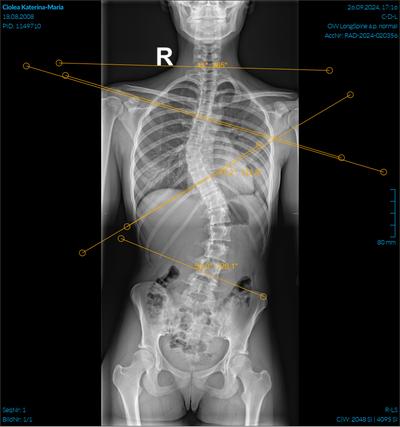
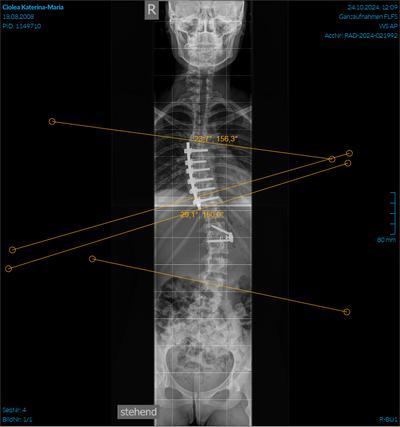
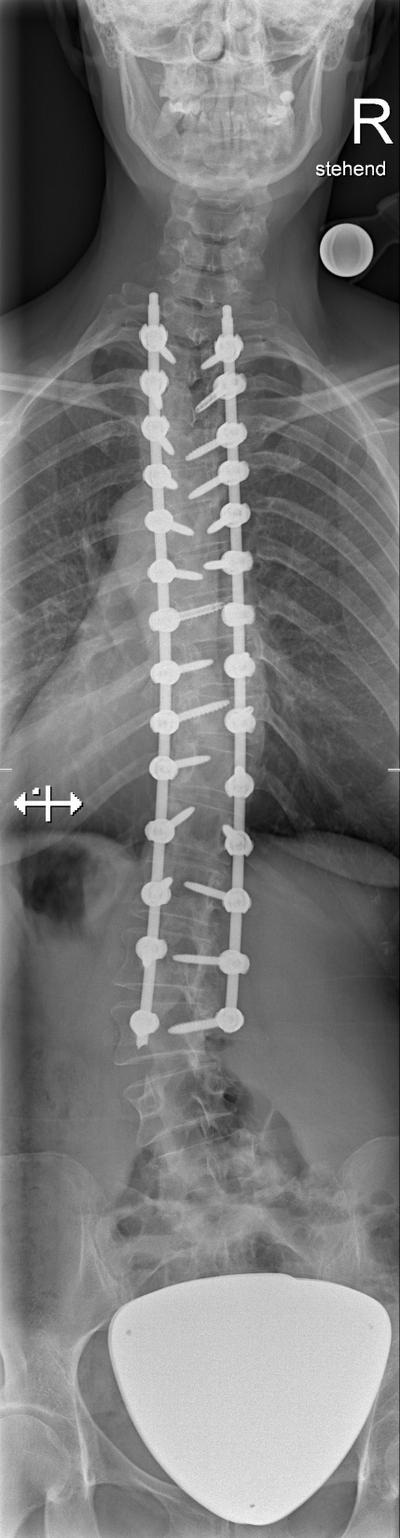
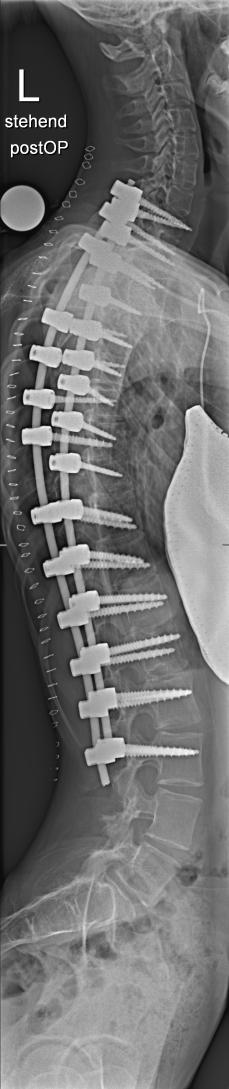
16 y.o., F, AIS Lenke 4B-.
Staged procedure with ventral release T6-11, halogravity traction and dorsal instrumented fusion T2-L3
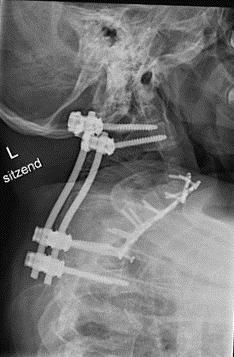
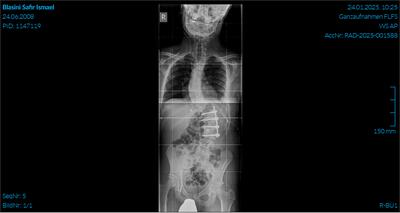
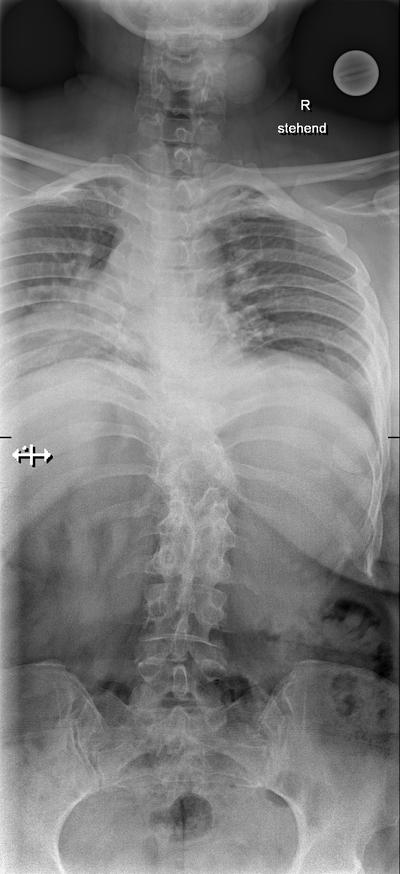
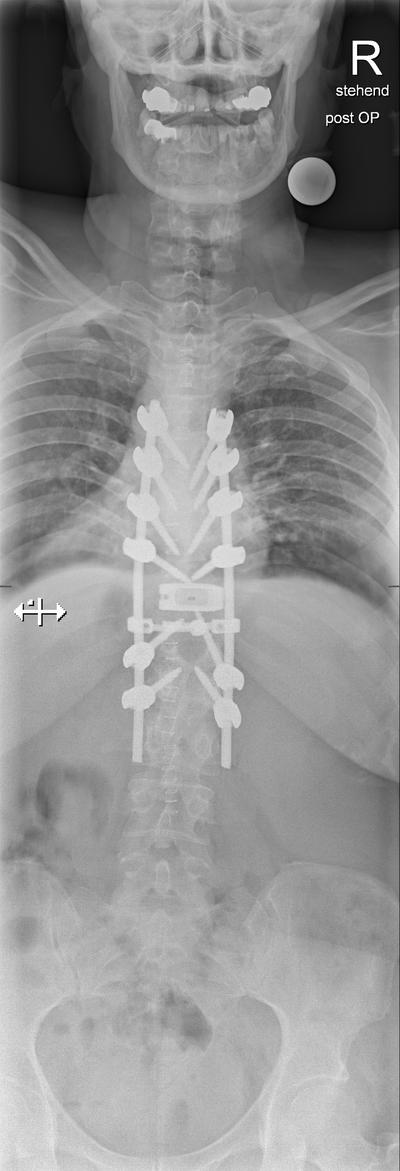
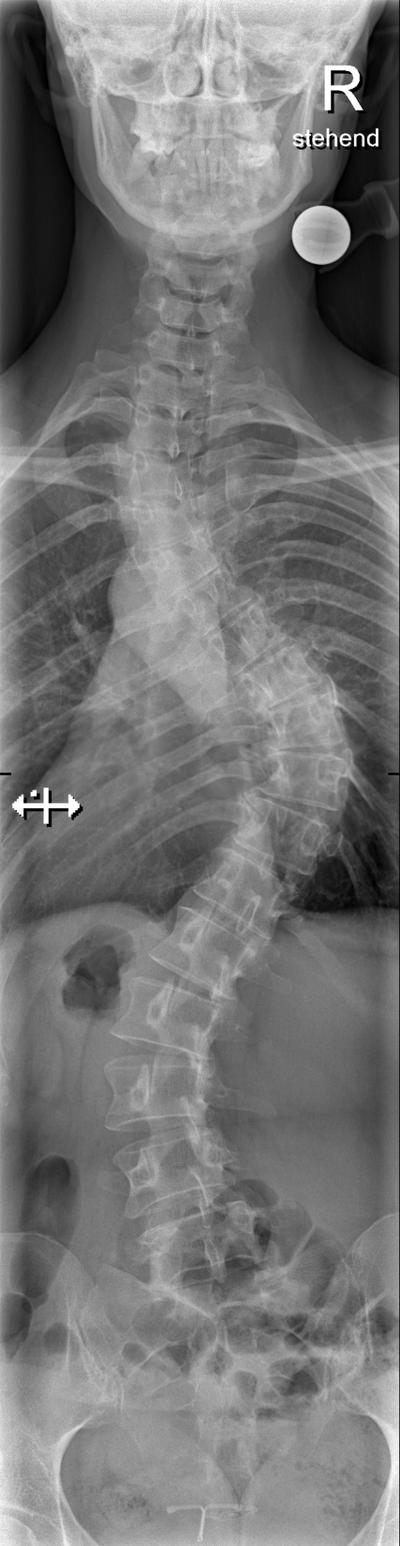
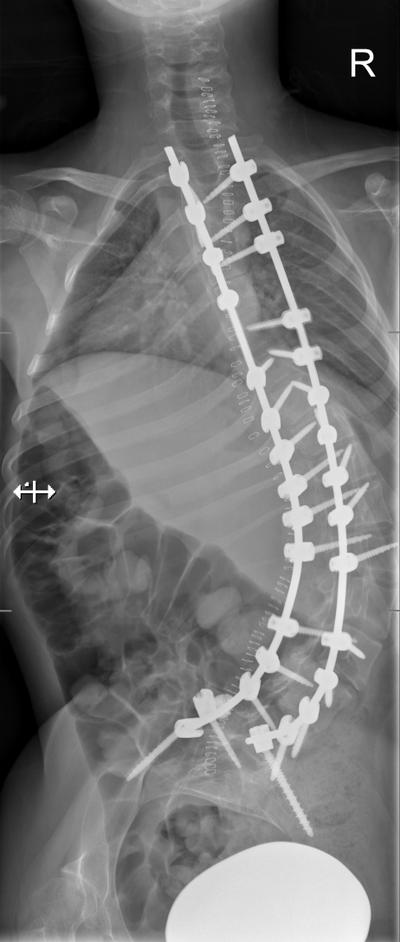
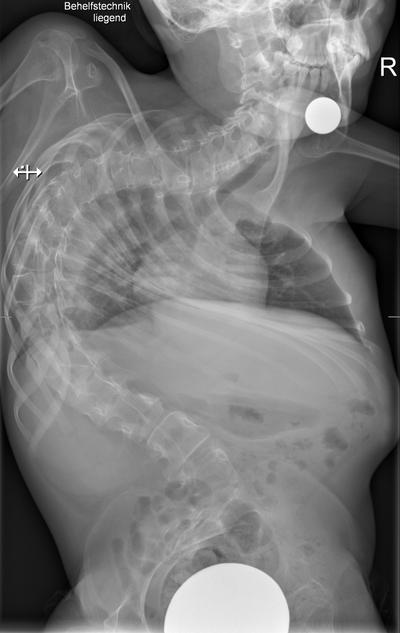
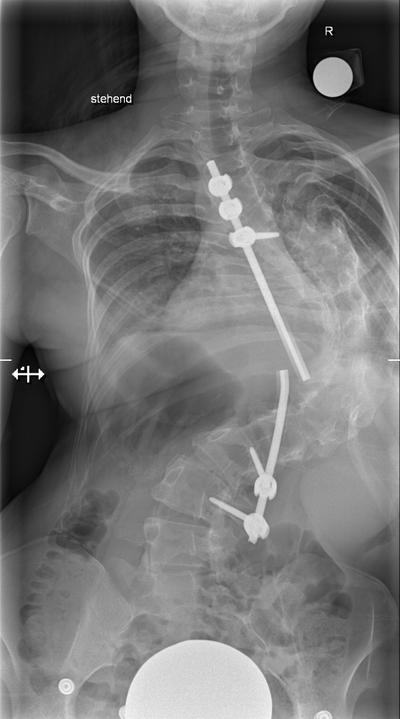
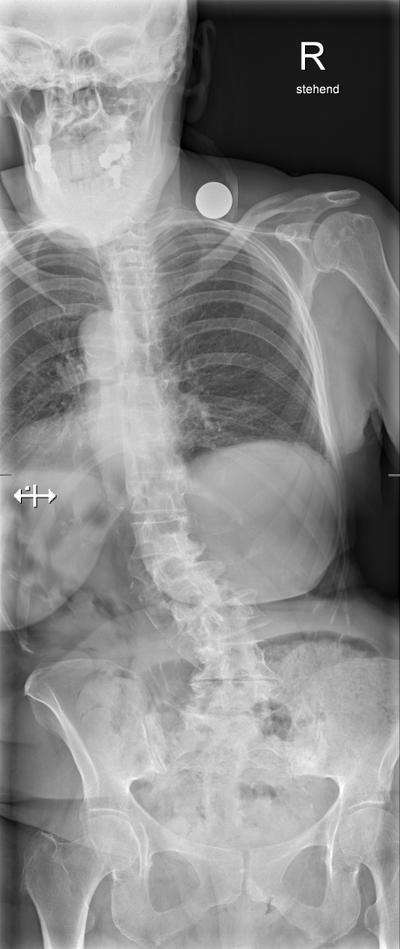
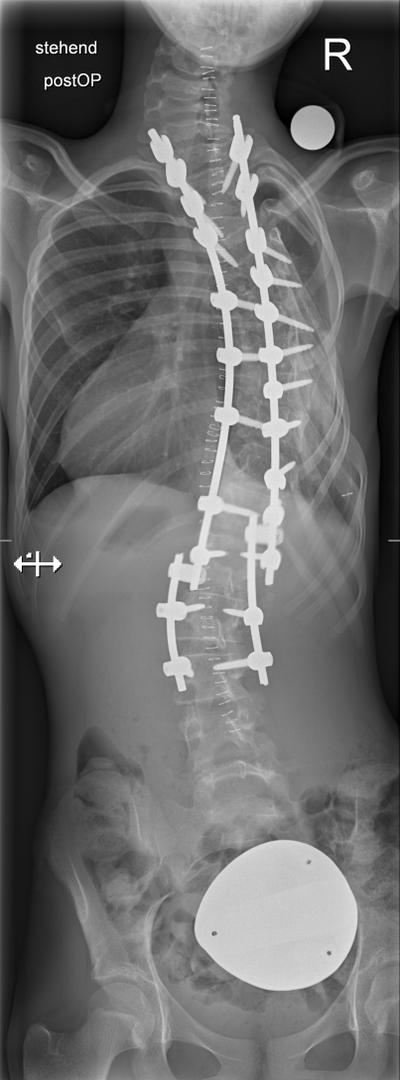
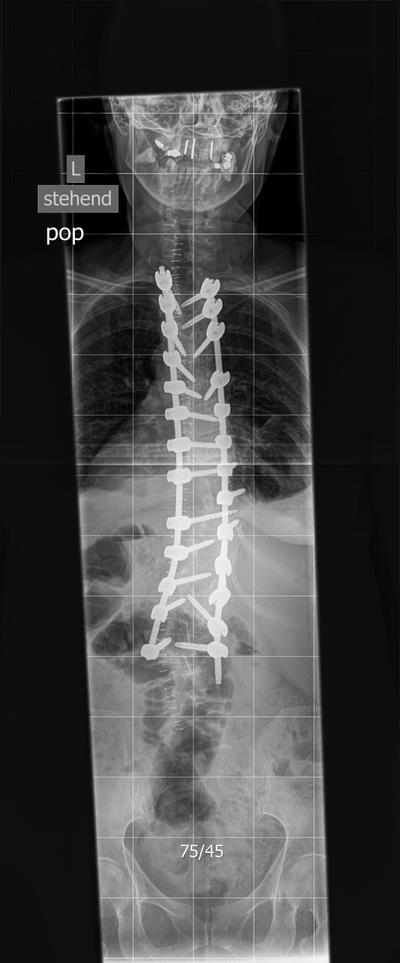
13 y.o. with severe idiopatic scoliosis Lenke 4B+.
Staged procedure with 1.ventral release T4-T11, halo-traction, 2.dorsal release and screw-placement, again halo traction and finally 3. instrumented fusion T1-L3
00.00.2020
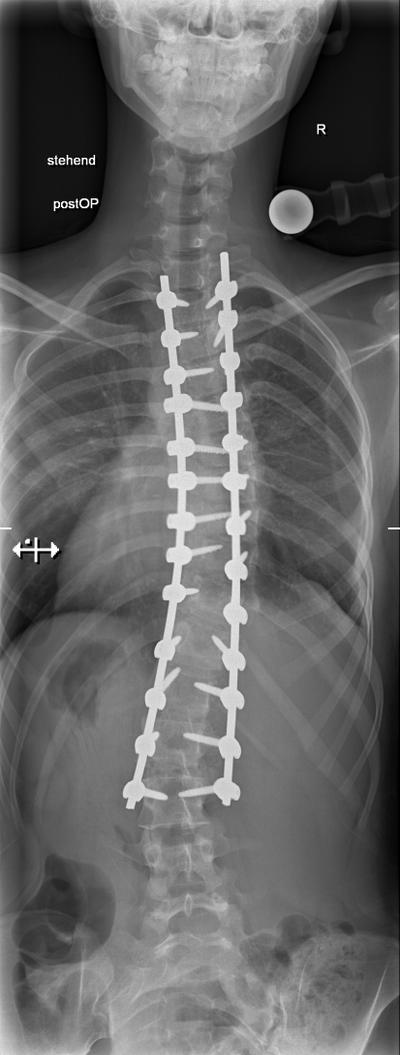
16 y.o. girl Lenke 3A-. Staged procedure with 1.ventral release T5-10 and 2.dorsal release and instrumented fusion T2-L3. Note the marked apex derotation as shown by rib re-alignment postop
9
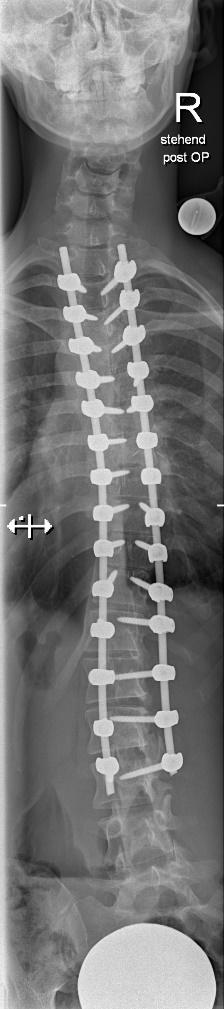
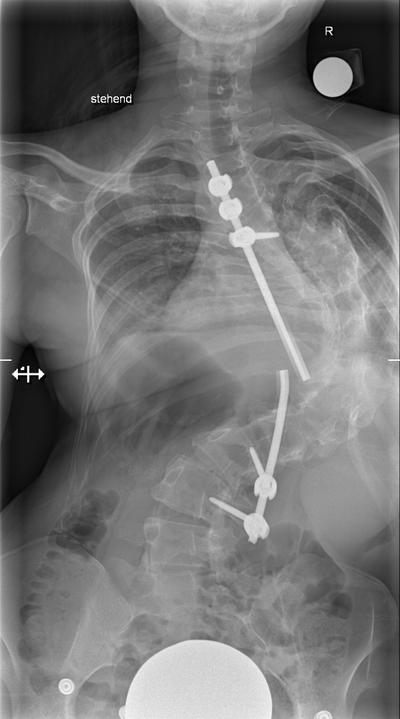
Idiopathic scoliosis Lenke 3 C- in a 28 y.o. mother.
Postop after1. ventral release T5-11 and 2.dorsal instrumented fusion T2-L3 in separate sessions. The LIV retained some rotation with L4 spared
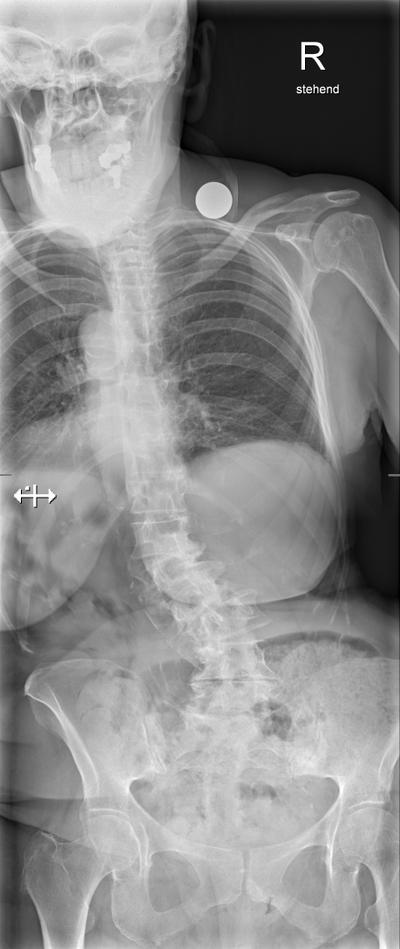
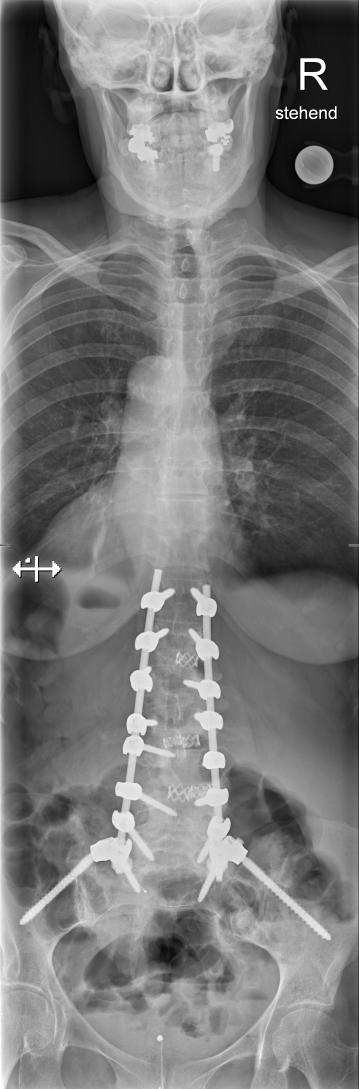
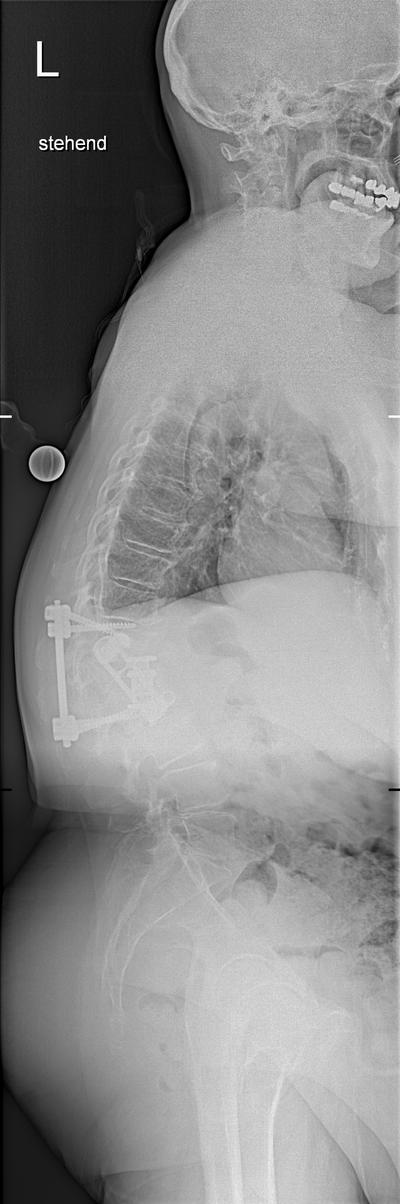
55 y.o. with AIS, stiff thoracic curve with apical spontaneous fusion. Staged approach with ventral release and subsequently dorsal instrumented fusion T2- L3
17, F, AIS, first operation elsewhere, partly fused, 1. removal of fixation and dorsal release, 2.Halotraction, 3.ventral release and 4. dorsal instrumented fusion
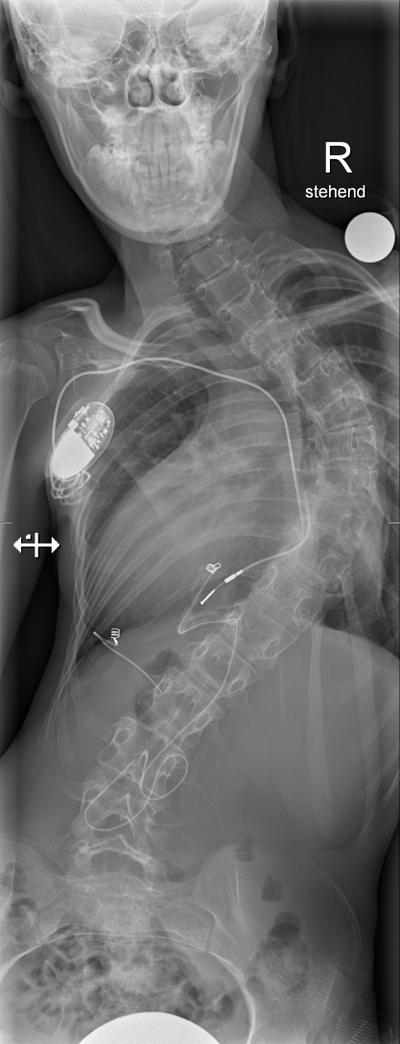
15, F, 1.dorsal release, 2.halogravity, 3.fusion. No ventral release because of impaired heart and pulmonary function.
13 y.o. girl Lenke 1 B -. Should one do a ventral release and then fuse dorsally (LIV would be in the best case scenario L3) or go for a selective thoracic fusion? Ventral, dorsal or combined?
After ventral kyphosing derotation and selective thoracic fusion T5-T11. Postop the lumbar curve decreased from 55 to 19 degrees, we got some decent thoracic kyphosis and subsequently reduced the compensatory cervical kyphosis.
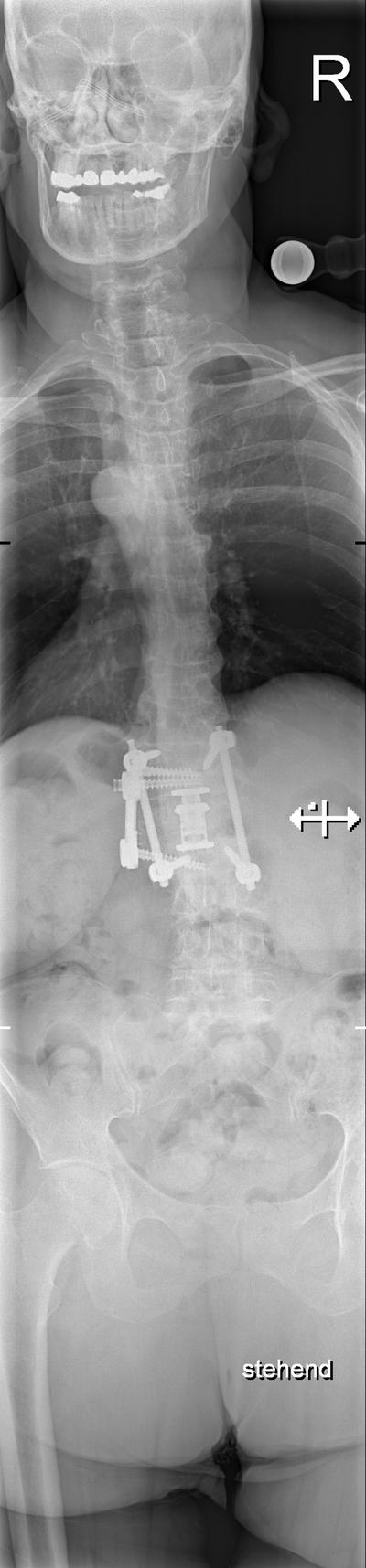
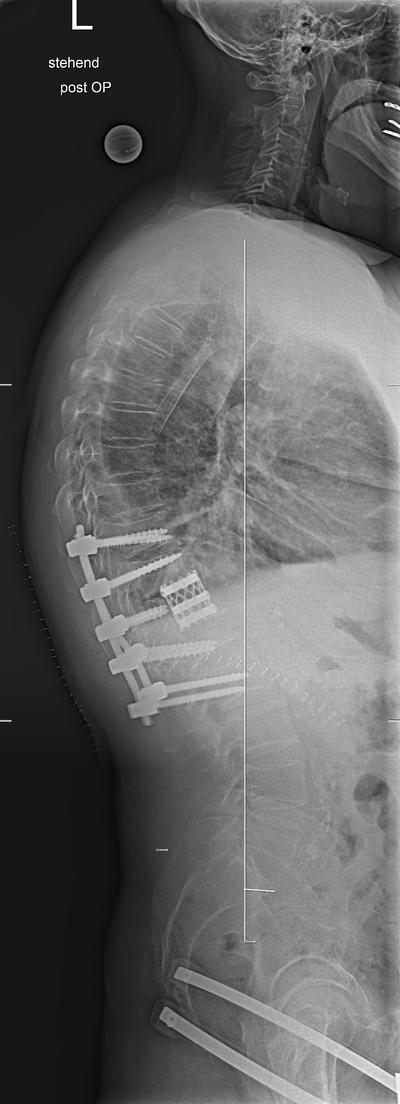
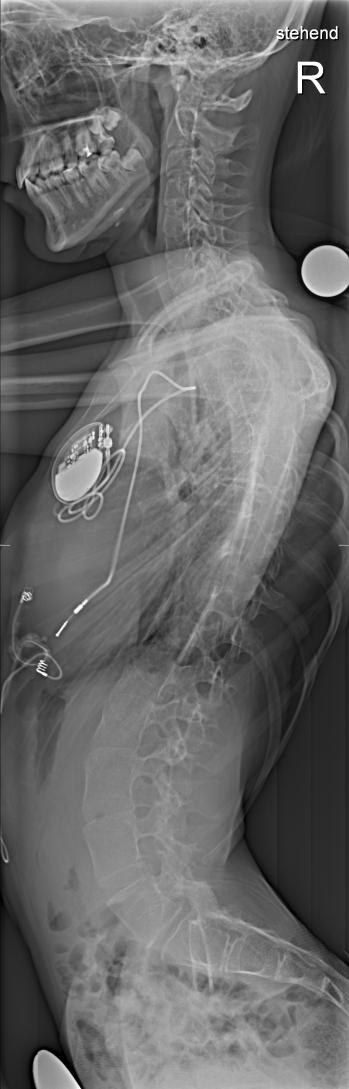
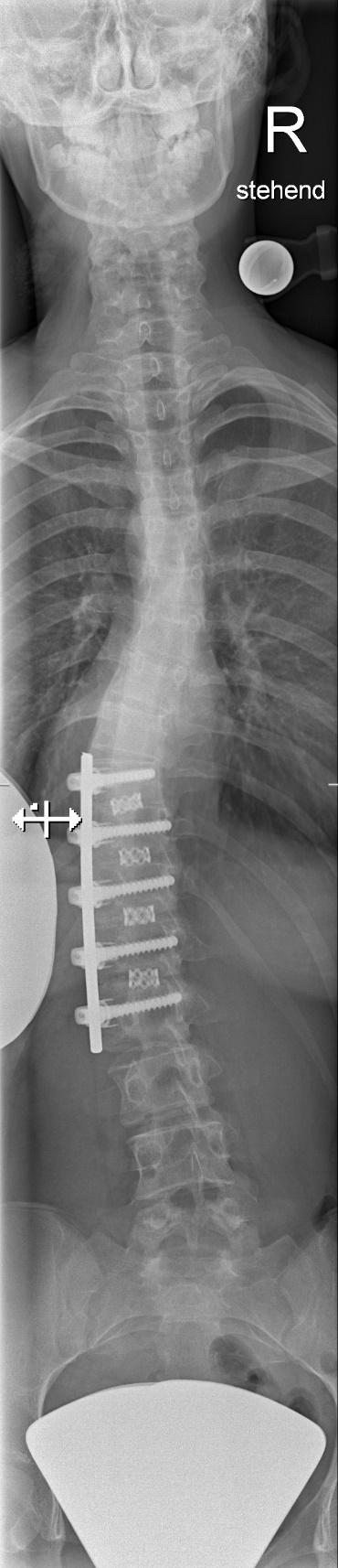
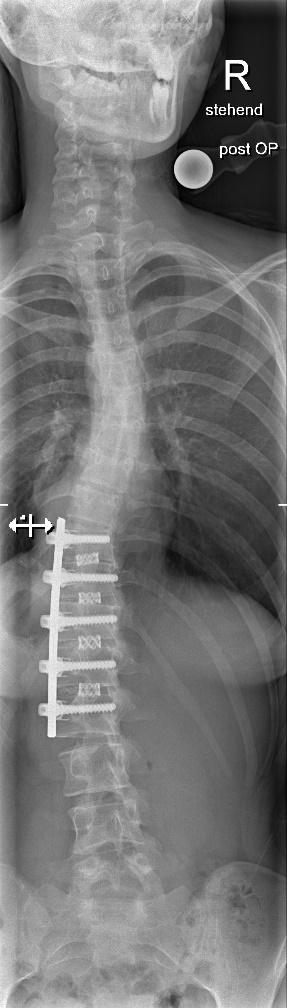
15 y.o girl AIS Lenke 1CN. Proximal thoracic and lumbar curves corect just underneath 25°. Significant rotation of lumbar vertebrae
Short fusion T10-L2 through open thoracofrenolumbotomy. The lateral approach simply allows better derotation.
Promises (unfulfilled?) for the futureAIS Lenke 6 in 12 y.o. Shilla growth-guidance instrumentation
Promises (unfulfilled?) for the futureVertebral body tethering (VBT) – trade mobility for predictability?